What is HoLEP Surgery?
HoLEP surgery is an effective and new method in the treatment of benign Prostatic Hyperplasia. Benign prostate hyperplasia, also known as BPH in short, is one of the most common urological diseases in elderly men after 60 years of age and is a benign version of the prostate that does not turn into cancer. Benign Prostatic Hyperplasia is a benign condition, meaning it is not cancer. In this disease, if the complaints are not too many at the beginning, drug treatment is sufficient and the patients are usually relieved by drug treatment. However, over time, complaints increase and drug treatment becomes ineffective and surgery is required.
HoLEP, which is the abbreviation of Holmium Laser Enucleation of Prostate, is a benign prostate surgery performed with laser to remove the enlarged part of the prostate using holmium laser.
How is HoLEP Surgery Done?
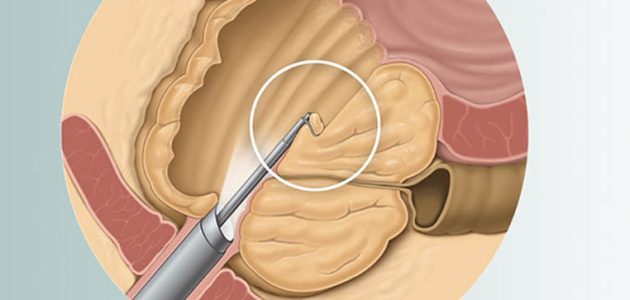
The HoLEP method is to enter the urethra with special endoscopic instruments (optical and illuminated system) and push the parts of the prostate (adenoma) that press on the urethra (urinary canal) from the capsule (prostate membrane) by laser and push them into the bladder. and it is an operation performed in the form of separating and removing prostate pieces into very small pieces with a system called morcellator.
In this system, there are no incisions or surgical scars in the body. Postoperatively, a Foley catheter is inserted in the patients and remains for 2 days. The procedure is performed with general or spinal anesthesia.

- Bu yöntemi ile kanama diğer yöntemlere göre daha az olur,
- HoLEP ameliyatı sonrası hastalar daha az hastanede yatar, daha erken taburcu olur,
- Ameliyat sonrası hastalar normal hayatlarına daha erken dönerler,
- İşlem sonrası hastalar daha az sondalı kalır,
- Bu yöntemle yapılan ameliyatta daha fazla prostat dokusu çıkartılır
- Daha fazla prostat dokusu çıkartıldığından çıkartılan parçaların incelenmesi sonucu prostat kanseri yakalama ihtimali daha yüksektir,
- Bu yöntemle prostatın tekrarlama oranı yoktur, son derece azdır
- TUR ameliyatında görülen “TUR sendromu” HoLEP ameliyatında görülmmez,
- Laser yöntemi ile ameliyat sonrası cinsel fonksiyonlar etkilenmez. Çünkü lazer enerjisi çok derine nüfuz etmediğinden penisin ereksiyon sağlayan sinirlerine hasar daha az bir ihtimaldir. Oysa diğer yöntemlerde değişik derecelerde cinsel fonksiyon bozuklukları görülür,
- Her büyüklükteki prostatlarda uygulanabilir,
- Bu yöntemle ameliyat sonrası mesane boynu darlığı diğer yöntemlere daha seyrek görülür,
- Tüm bu avantajlarından dolayı HoLEP yöntemi iyi huylu prostat tedavisinde “altın standart” tedavi yöntemi olarak kabul edilmektedir.
Is Prostate Biopsy Required for Every Patient for HoLEP Surgery?
Prostate surgery with the HoLEP method is performed in benign Prostatic Hyperplasia. However, it is important to determine in advance that the patients who will undergo this surgery do not have prostate cancer. Because if cancer comes out, the type of surgery changes.
Most of our patients are wondering whether preoperative prostate biopsy will be necessary with this method. In patients who will undergo surgery for benign prostatic hyperplasia (BPH), it should be demonstrated that they do not have prostate cancer.
Investigations before HoLEP surgery to find out if there is prostate cancer;
- PSA test: Normal PSA values are between 0-4 ng/ml, if it is above this, it is necessary to differentiate cancer with other methods.
- Prostate examination: The rectal examination of the prostate with fingers gives general information about whether there is prostate cancer.
- Prostate multi-parametric MR film: This is a special MRI method and gives high information if there is cancer in the prostate. Here, the suspicious lesion in the prostate is evaluated on a scale of 1-5 with a scoring method called the PIRAD system. If the result is PIRAD 4-5, the probability of cancer is high and a biopsy should be taken. At values below this, there is no need for biopsy as the probability of cancer will be low.
- Prostate biopsy: The definitive diagnosis of prostate cancer is made by biopsy. The biopsy (part) taken from the suspected cancer is examined pathologically and it is clearly understood whether there is cancer or not.
In a study conducted in 2021, 397 patients who would undergo HoLEP surgery were examined, and as a result of the analysis of the data obtained from them, it was explained in detail which patients would be required to undergo further study for prostate cancer.
The patients were examined in 2 groups and the patients who had the standard examination, only the finger examination and the PSA test were requested. The patients in the second group were classified as the advanced study group patients. Multiparametric prostate MRI and biopsy were performed on patients in the advanced research group.
Based on the data from this study, the authors came to some conclusions about pre-HoLEP biopsy. We can summarize them as follows.
Conditions for prostate biopsy before HoLEP
- Prostate biopsy is not required for every patient who will be treated with the HoLEP surgery method due to BPH.
- If patients have high PSA values, prostate multiparametric MRI should be requested. If the PI-RADS value is 4/5 as a result of MRI, prostate biopsy should be taken because the risk of cancer in these patients will be high. A biopsy is not required if there are lower PIRADS scores.
- In addition, if 2 or more biopsies have been taken beforehand in patients with elevated PSA and no prostate cancer has been found as a result, the risk of cancer is very low in these patients and biopsy is not required.
HoLEP surgery is performed in three main ways!
- Three lober prostatectomy: With this method, an incision (incision) is made by entering the urethra, starting from the bladder side at the 5 and 7 clockwise direction in the prostatic urethra, and up to the prostate capsule, to the lower part of the prostate, called the verumontanum. Then, the middle lobe of the prostate from the verumontanum to the bladder is separated from the capsule and pushed into the bladder. Then, the right and left prostate lobes are separated from the capsule (dissection) and pushed into the bladder in the same way. In this method, because the prostate is dissected from the capsule in 3 parts (separation from the prostate capsule) and pushed into the bladder, it is called “three lobar prostatectomy” in English (in 3 parts). These pieces, which are thrown into the bladder, are then taken out in very small pieces with a device called a “morcellator”.
- Two lober prostatectomy:In this method, the enlarged prostate adenoma is separated from the prostate membrane in 2 pieces and thrown into the bladder, and from there it is fragmented with a morcellator and taken out in very small pieces without making any incisions in the body.
- En block prostatectomyIt is the method of separating the enlarged prostate adenoma from the capsule of the prostate and throwing it into the bladder. Here, the benign prostate tissue, which makes urination difficult, is separated from the capsule as a whole and thrown into the bladder, and then it is broken up with a “morcellator” and taken out in very small pieces.
After the prostate is taken out with all three methods, bleeding is controlled with laser energy, small vessels are burned, and finally, the patient is terminated by placing a catheter in the urinary canal called a Foley catheter.
All three methods have no superiority or advantage over each other. The process is exactly the same. The choice is all about the surgeon’s habit.
BPH and HoLEP laser therapy
BPH (benign prostate hyperplasia), is benign Prostatic Hyperplasia, a disease that occurs in more than 40 percent of patients aged 60 years and older. BPH is a benign disease and its treatment is different from prostate cancer. Benign Prostatic Hyperplasia in older men usually presents with urinary complaints.
Urinary complaints due to Prostatic Hyperplasia are as follows:
HoLEP surgery in urology is a laser surgical method that is effective in benign enlargement of the prostate. Common complaints in elderly male patients with benign Prostatic Hyperplasia include:
- Frequent urination, especially at night
- Difficulty to urinate, needing to strain
- Drops of urine at the end of urination
- Forked urination
- Urinary incontinence before reaching the toilet with the feeling of sudden urination
- The need to urinate again after urinating
- Feeling of incomplete emptying of the bladder after urinating
Which patients need HoLEP surgery?
There is no need for surgery for every patient with Prostatic Hyperplasia. Some of the men with enlarged prostate usually respond well to drug treatments called alpha blockers if their complaints are not too severe and do not need surgery. However, over time, patients begin to not benefit much from these drugs, and in such cases, we have no more options than surgical treatment.
The most commonly used methods in the surgical treatment of benign Prostatic Hyperplasia: Open prostate surgery, TUR-P (transurethral resection of the prostate), and Plasmakinetic are known surgical methods. However, with the advancement of technology, serious progress has been made in prostate surgeries performed with laser. In recent years, holmium laser closed surgery of the prostate (HoLEP) has been used as an effective treatment method in developed western countries.
Patients requiring HoLEP therapy
In some cases with Prostatic Hyperplasia, drugs are insufficient and surgical treatment is absolutely necessary. We can summarize the situations that absolutely require surgery (including HoLEP surgery) as follows:
Various drug groups are used to treat symptoms associated with BPH.
- Patients for whom drug therapy is not effective: While patients benefit from drug therapy in the past, these drugs become ineffective as time progresses and surgery is required. In elderly patients, the effect of drugs may be less, in these patients, if drug therapy is not effective and the general condition of the patient is suitable for surgery, surgery should be performed.
- Serious diabetics: Nerve damage, called neuropathy, develops in diabetic patients over time, and these patients cannot see the expected benefit from drug treatments as the bladder neck and bladder nerves will be damaged.
- Inward enlargement of the prostate: The prostate enlarges into the bladder in some patients. This is called median or middle lobe hyperplasia, and in these patients, medications are often not effective and surgery is required.
- Patients who urinate frequently at night: Since patients urinate frequently at night, their sleep patterns are disrupted and this reduces the quality of life of people in their normal daily lives. For this reason, it is appropriate for patients who suffer from insomnia due to Prostatic Hyperplasia and whose daily social life and work life are adversely affected to undergo surgery.
- Excess urine remaining in the bladder after urination: Inability to empty the bladder completely after urinating and excess urine remaining in the bladder is another reason for surgery. Normally, after urinating, the bladder, that is, the urinary bladder, should be completely emptied. If 100-150 cc or more of urine remains in the urinary bladder, this is a reason for surgery.
- Frequent urinary tract infection: Due to the pressure on the urinary canal (urethra) due to Prostatic Hyperplasia, patients cannot fully empty their bladders and as a result, residual urine remains in the bladder, which leads to recurrent urinary tract infections. The definitive solution for such infections that cannot be controlled with antibiotics, is prostate surgery.
- Bladder stones: Incomplete emptying of the bladder and excess urine remaining in the bladder after micturition cause stone formation in the bladder over time. Stones can be numerous. Removing the stones in the treatment is not the solution, the definitive solution is prostate surgery.
- Inability to urinate: In some prostate patients, the urinary canal (urethra) is completely closed due to the prostate and patients cannot urinate, a catheter must be inserted. In these patients, the definitive treatment is surgery instead of medication.
- Bleeding from the bladder: Due to Prostatic Hyperplasia, there is enlargement of the veins in the bladder neck, and in some cases, these enlarged veins open and cause serious bleeding. In such patients, drug therapy is not effective as a treatment method.
- Impaired kidney function (kidney failure): In patients with long-term Prostatic Hyperplasia and severe obstruction, enlargement of the ureter and kidneys (hydroureteronephrosis) develops over time and, if these patients lose more time and do not undergo surgery, renal failure may result.
- Bladder diverticulum: In patients with BPH, in case of incomplete emptying of the urinary bladder and the progression of the obstruction, outward herniation in the urinary bladder occurs over time, these are called “diverticulum”. These diverticula can be numerous and in different sizes. In such patients, the definitive treatment is surgery instead of drug therapy.
Patients not eligible for HoLEP
HoLEP surgery is an operation that can be performed on any patient with benign Prostatic Hyperplasia, provided that it is very careful. However, in some cases, it is necessary to be more careful and prepare accordingly.
- Patients with serious bleeding problems: In patients with serious bleeding problems, it is more appropriate to perform the procedure after the necessary treatments (if surgery is required).
- Patients who previously havehad prostate surgery: HoLEP method is performed in patients who have had prostate surgery before and whose prostate cannot be completely removed, but if the remaining part is very small and the patient has a high cost with this method, the remaining small parts can be removed with other methods (such as TUR). Prior surgery is not a definite obstacle. We have patients that we have successfully done in this way.
- Patients who cannot be positioned for surgery: Operations such as TUR, HoLEP, plasmatinetics are difficult for technical reasons in patients who have problems in the leg joints and cannot be positioned appropriately for surgery. Because in these surgeries, the patient must be in a special position, if there is a serious problem in the hip joints and the joints cannot be broken, there will be difficulty in the surgery.
Preparation before the HoLEP
HoLEP surgery is a surgical procedure like other surgeries. It is done in operating room conditions. Patients who are decided to have surgery are evaluated in detail by the anesthesiologist.
Urological evaluation of patients
Patients who will have HoLEP surgery are subjected to a detailed urological examination.
For this reason:
- Prostate examination is done from the anus with fingers
- Prostate cancer should be distinguished.
- PSA (prostate specific antigen) test should be done, if it is high, further research should be done in terms of cancer. For this purpose, multiparametric MRI and prostate biopsy should be performed according to the result.
- Kidneys and bladder should be evaluated: Information about kidneys and bladder can be obtained by performing ultrasonography and kidney function tests.
- If necessary, tests showing bladder functions such as urodynamics may be ordered.
- Performing the uroflow test, which shows the urine flow, gives an idea about the urine flow.
- Determination of residual urine after voiding in the bladder:Normally, there should be no urine left in the bladder after urinating, but if there is a blockage, varying degrees of urine will remain in the bladder.
- Urinalysis should be done:If there is an infection, it should be treated with appropriate antibiotics before surgery.
General evaluation of the patient
Patients who will undergo HoLEP surgery undergo a general evaluation before surgery. For this purpose, routine blood tests are requested from patients and:
- Liver-kidney function tests are requested
- Bleeding and coagulation tests are checked to see if they are normal.
- Routine blood count is done, blood group is determined. If the blood values are insufficient, the patient is made suitable for anesthesia by giving blood beforehand.
- Chest X-ray is taken
- EKG is taken to find out whether the lungs and heart are normal, and if necessary, necessary precautions are taken in advance.
- If the anesthesiologist deems it necessary, consultations are requested from the relevant departments for patients with chronic problems such as heart, lung or diabetes, and necessary treatments are performed according to the recommendations received from these departments.
- If patients are taking anticoagulants before, they are usually discontinued one week before surgery or replaced with more suitable ones.
- If patients are using diabetes medication, blood pressure medication or chronic medication due to neurological disorders, it would be beneficial for the anesthesiologist to know these before the operation. It is generally recommended that blood pressure and diabetes medications be taken in the same way. Other medications may need to be discontinued before surgery.
What patients should do before surgery
- The patients fast after 24.00 the night before the operation and do not eat or drink anything by mouth (at least 5-6 hours before the operation),
- If there are blood pressure and diabetes medications that he used before, they are used in the same way if they are approved by the relevant specialist or anesthesiologist.
- Before the surgery, sedative drugs can be given to the patients to relax and to enter the surgery without stress,
- Daily hospital clothes (slippers, pajamas, etc.) to be used before coming to the hospital are provided,
- After the pre-operative identity check and hospitalization, an “informed consent form” about the surgery is signed,
- It is recommended to have as few visitors as possible, short visits and only one accompanying person.
Information about the surgery
- The patients are in the supine position and the operation is performed under general or spinal anesthesia,
- After the surgery, a Foley catheter is inserted through the urinary tract to the patient,
- The duration of the operation varies according to the size of the prostate, and if it is not very large, the operation can be completed in 1-2 hours. But in large prostates, the duration may be longer.
Postoperation
- After the surgery, patients are kept in the operating room for 20-30 minutes until they feel well and then go to their room.
- Patients are not given food or drink orally for 4-5 hours after the operation. During this period, only serum is given intravenously.
- Painkillers and antibiotic prophylactic treatment against infection are started to relieve the patient’s pain. (intravenous or by injection).
- After 5 hours, the patient is evaluated and if there is no problem, he starts to take water and watery foods by mouth. He slowly gets up and walks. If he has had spinal anesthesia, he will be walking later.
- On the first day after the operation, the patient is evaluated and the vascular access is cut. He starts to be fed orally and his drugs are given in the form of oral pills instead of veins.
- Patients are advised to drink plenty of water after starting to take it orally. Drinking at least 2-3 liters of fluid a day is beneficial, and in this way, the urine color becomes lighter and there is no bleeding inside.
- If the general condition of the patients is good and there is no problem in urination, they are discharged on the first or second day.
- Painkillers and antibiotic treatment are started for the discharged patients to take them orally.
- The urinary catheter is usually removed on the 2nd day. If patients also have urethral stricture and it has been treated, or sometimes in fatty patients, the catheter can be withdrawn in the following days.
Advantages of prostate surgery with the HoLEP method compared to other methods
There are prostate TUR, plasmakinetic, rectum surgeries and open prostate surgery similar to HoLEP surgery, but HoLEP surgery has many advantages over these surgeries. Due to these advantages, this method in the surgical treatment of benign Prostatic Hyperplasia is currently considered as the “gold standard treatment method“. In other words, it is a surgical method with the best effectiveness and the least side effects.
- With this method, bleeding is less compared to other methods,
- After HoLEP surgery, patients are hospitalized less often, discharged earlier,
- After the surgery, patients return to their normal lives earlier,
- After the procedure, patients remain less probe,
- In the surgery performed with this method, more prostate tissue is removed.
- Since more prostate tissue is removed, the probability of catching prostate cancer is higher as a result of the examination of the removed pieces,
- With this method, there is no recurrence rate of the prostate, it is extremely low.
- “TUR syndrome” seen in TUR surgery is not seen in HoLEP surgery,
- In the surgery performed with the laser method, sexual functions are not affected after the surgery. Because laser energy does not penetrate very deeply, damage to the erectile nerves of the penis is less likely. However, in other methods, various degrees of sexual dysfunction are seen.
- It can be applied to prostates of all sizes,
- With this method, postoperative bladder neck stenosis is less common than other methods,
- Because of all these advantages, the HoLEP method is accepted as the “gold standard” treatment method in the treatment of benign prostate.
Surgical treatment of benign prostate disease with the HoLEP method is very popular today. For a long time, transurethral resection of the prostate (TUR-P) was the gold standard method for the surgical treatment of benign Prostatic Hyperplasia. Today, HoLEP is accepted as the gold standard treatment method in the treatment of Prostatic Hyperplasia. While other methods vary according to the size of the prostate, HoLEP is a method applied to prostates of all sizes.
Although HoLEP surgery has been popular in the last few years, it is not actually a new method. It is a well-known technique that has been used for nearly 20 years. The first prostate surgery was performed with this method in the late 1990s. With the advancement of the technique over time, it has become popular only today. Another reason why the method has not become widespread is the long learning curve. Besides the long learning time, the expensiveness of the system is another reason why HoLEP is not widely used.
There have been significant advances in laser technology in the nearly 20 years since it was first implemented. Prost with laser Since it was first applied, there have been serious advances in laser technology in about 20 years. The process after pushing the prostate tissue into the bladder as well as the separation of the prostate tissue from the capsule with the laser is a very important step.
The disintegration of the tissues in the bladder, that is, the “morcellation” process, requires a separate system. Prostate tissues in the bladder are broken down by a system called “morcellator”. This system is very developed today, and in this way, the prostate, which is thrown into the bladder, is quickly divided into small pieces and taken out.
The duration of the operation varies from patient to patient. The larger the prostate, the longer the operation time. In patients with large prostates, the operation time takes longer for two reasons. First, the separation of the prostate from the capsule takes a long time. Another is the disintegration process of the prostate thrown into the bladder, that is, morcellation takes a long time.
Apart from these, sometimes in small prostate patients, if a biopsy has been done before or if there is an infection, adhesions may occur due to these and the surgery may be prolonged.
One of the frequently asked questions by patients is whether HoLEP surgery is associated with prostate size. I will describe the summary of an article about the HoLEP method published in the Canadian Urology journal. Various techniques applied in the study, safety, efficacy, complications, etc. have been extensively studied.
The prominent findings of the study can be listed as follows:
- HoLEP can be applied to prostates of all sizes.
- Large or small prostate is not an obstacle for surgery.
- There is very little bleeding in this method.
- Patients are hospitalized less
- Remains with shorter probe after surgery
- They return to their daily lives earlier
- Rapid improvement in urine flow
- Recurrence is extremely low
In conclusion, the HoLEP method is an extremely safe and effective method in the treatment of benign Prostatic Hyperplasia. It is suitable for prostates of all sizes.
Prostate size or smallness is not an obstacle for surgery. The American and European Associations of Urology (AUA, EAU) have accepted the HoLEP method as the gold standard method in prostate treatment.
Today, the most commonly used surgical methods in the treatment of BPH are:
- TUR (transurethral resection of the prostate) surgery
- Plasmakinetics –TUR
- Bipolar–TUR
- Monopolar –TUR
- Open prostate surgery in very large prostates
- HOLEP
- Other less commonly used surgical methods
As in all fields, new techniques and methods in medicine are changing rapidly day by day. HoLEP (holmium laser enucleation of the prostate) method, which is accepted as the newest and “gold standard” in the surgical treatment of benign prostate disease, is one of the newest surgical methods in the field of Urology.
Here, prostate tissue, which has grown by using laser and makes it difficult to urinate by pressing on the urinary canal, can be entered through the urinary canal and removed without any incision.
To briefly summarize;
Since patients with open prostate stay in the hospital longer, the price is higher for them. Bleeding and the need for blood transfusion are absent or extremely rare in HoLEP surgery compared to TUR and open prostate surgeries.
HoLEP patients stay on catheters for less time and stay in hospital for less time compared to other methods.
What should be considered after HoLEP?
HoLEP is a benign Prostatic Hyperplasia (BPH) surgery performed with a laser by entering through the urinary canal with a closed method. In this surgery, there is no incision or scar on the body, it is an endoscopic or closed method. Although there is no incision in the body in HoLEP surgery, there is an operation area made with laser in the prostate region. After the surgery, a Foley catheter is inserted and removed after 1-2 days, and the patients begin to urinate normally.
As in every surgery, there are some points to be considered after the surgery in HoLEP surgery. By paying maximum attention to these situations, possible complications, that is, side effects, are reduced. Bleeding is one of the most important issues to be considered after HoLEP and other closed prostate surgeries.
We can list the points that need to be considered in order to minimize or not at all the possibilities such as bleeding, inability to urinate, urinary tract infection:
- Sitting on a hard floor should be avoided as much as possible in the early postoperative periods,
- Do not sit for a long time, especially on hard ground,
- Care should be taken not to become constipated,
- In the first days after the surgery, patients should urinate frequently without waiting for urination,
- After the catheter is removed, it should be seen whether the patients urinate normally or not. Sometimes patients may not be able to urinate due to edema and small blood clots at the surgery site. In this case, the doctor should be informed and a catheter should be inserted if necessary. Such conditions can occur, albeit very rarely, especially in the very old and those with diabetes. By inserting the catheter, patients remain with the catheter for a few days and then urinate normally.
- Urinary incontinence may occur, especially in elderly patients, after the catheter is taken at first, while moving, sitting and getting up, and working. This situation is temporary and will mostly improve over time.
- Do not strain too much while urinating or making bowel movements.
- Avoid spicy food and drinks
- Heavy physical activity should not be done, excessive weight should not be lifted
- It should be protected from extreme cold for the first 2-3 weeks and rested in a warm environment.
- Burning during urination and dark urine are possible in the early periods after the catheter is taken, and these conditions are improved by increasing fluid intake.
- As with all post-operative surgeries, constipation may occur due to the effect of anesthesia after prostate surgeries. This situation is temporary, returns to normal in a few days. During this period, patients should be careful and do not strain too much, otherwise bleeding may occur due to excessive straining. In the early stages, drugs can be given to help patients perform defecation more easily.
- Fluid intake should be increased: Daily fluid intake should be kept around 2-3 liters
- Antibiotics and other drugs given should be used regularly
- Blood thinners should not be used unless necessary
- Since there is no incision or wound in the patients, they can take a bath with warm water after the catheter is removed after the surgery.
- In the first 7-10 days after the operation, the car should not be used, especially on long journeys.
- Avoid alcohol and excessive coffee consumption
- Urinary tract infections can be seen in patients. If there are complaints such as burning, turbid urine during urination, the patient should definitely consult his doctor or a urologist.
Benign Prostatic Hyperplasia (BPH) surgery with the HoLEP method is a gold standard method. In recent years, this method has become more widespread. One of the questions frequently asked by patients is “Does the prostate recur after HoLEP surgery?”. In addition, I will summarize the recurrence of the disease after surgery in comparison with commonly used methods.
Does HoLEP surgery negatively affect sexual functions?
Benign Prostatic Hyperplasia (BPH) in aging men is a common disease today. With the prolongation of life expectancy, there is an increase in the incidence of the disease. In the surgical treatment of benign Prostatic Hyperplasia, sexual problems appear in varying degrees depending on the procedure applied.
Commonly used surgical methods in the surgical treatment of BPH: Open surgery in very large prostate cases, TUR, plasmakinetic, bipolar and monopolar TUR surgeries and HOLEP (holmium laser enucleation of the prostate), that is, prostate surgery performed with laser, which has been used frequently in recent years and is accepted as the “gold standard” in the surgical treatment of benign Prostatic Hyperplasia.
We can examine the sexual (sexual) problems frequently seen at the end of the surgical treatment of the prostate in 2 main groups:
- Retrograde ejaculation (absence of semen, mixing with urine)
- Erectile dysfunction (erectile dysfunction, impotence)
Retrograde ejaculation
Normally, the bladder neck is panned during ejaculation and the semen is expelled from the urinary canal (urethra) by intercourse. During surgical interventions for bladder neck and benign prostate disease, the anatomy of the bladder neck is disrupted and the bladder neck cannot be closed during ejaculation. As a result, the semen cannot be expelled and escapes into the bladder, and the semen in the bladder is then excreted together with the urine. This situation is called “retrograde ejaculation”, the reflux of semen.
Retrograde ejaculation is undesirable by sexually active men, but it happens in almost all surgical methods used in the treatment of benign prostate. It has been reported that in surgeries performed with the HOLEP method, which has been used in recent years, semen retraction is less than other methods, but despite this, it should be noted before the operation that this possibility may still exist. Retraction of semen does not directly affect erectile functions in patients, but it can have a negative psychological effect. It is also important in this respect that patients are informed about this issue in advance.
The point where retrograde ejaculation is of primary importance is to be able to have a child. In cases where the semen recedes, it is difficult to have a child in normal ways after intercourse, but; With artificial insemination methods to be made with sperm obtained from urine after intercourse, patients can have children if they wish, or; It is possible for patients to have children with sperm taken from the testicles or epididymis (semen ducts), similarly with in vitro fertilization methods.
Erectile dysfunction
Erectile dysfunction (ED) or erectile dysfunction (impotence) is defined as “the inability to initiate or maintain a normal relationship”. One of the complications seen after benign Prostatic Hyperplasia surgeries is erectile dysfunction, that is, erectile dysfunction. The incidence of erectile dysfunction increases with age, and considering that the incidence of BPH increases with age, it is expected that ED problems are more common in prostate BPH patients.
Benign Prostatic Hyperplasia, erection problems as a result of surgical treatment varies according to the type of technique applied. This is because the nerves that go to the penis and are responsible for erection pass from the outside of the prostate adjacent to the prostate and can be damaged during these surgeries. In some of the surgical methods applied for BPH, post-procedure erectile functions are negatively affected to varying degrees. However, with the HOLEP method, which has been put into practice in recent years, it has been reported that erection problems do not deteriorate or even increase.
The reason for this is related to the laser energy source used in HOLEP surgery. Since the laser energy used in the HOLEP method penetrates to a depth of 0.4 mm, there is no negative effect on the nerves passing outside the prostate and adjacent to the prostate capsule, and as a result, erection problems are not seen in HOLEP patients.
Commonly used surgical methods in the treatment of BPH: Open prostatectomy, TUR, Greenlight
Open prostate surgery (open prostatectomy) and TUR surgery are two commonly used methods for surgical treatment in BPH patients. The most important negative side of these surgeries is that the parts of the prostate that are enlarged and press on the urinary canal cannot be completely removed, that is, their recurrence.
In some patients, prostate surgery is performed with the closed method using the greenlight laser method. In this method, enlarged prostate tissues are not removed, only vaporized. Since only the parts that close the urinary canal are evaporated with the evaporation method, a large part of the prostate remains and recurrence is frequent. Since the prostate is not removed, the complaints begin again in the future.
Another disadvantage of prostate surgery with greenlight laser is that tissue cannot be taken for pathological examination after surgery. Since a piece is not taken and sent to pathology with this method, if the patient has prostate cancer, this cancer is overlooked. However, in the HoLEP technique, the entire prostate is taken and sent to pathology for cancer analysis. Thus, if the patients have prostate cancer, it is revealed in the pathological examination.
Open prostate surgery is an old method used in the treatment of benign Prostatic Hyperplasia. Open prostate surgery is a frequently preferred surgical method in patients with very large prostates. With this method, prostate adenoma (prostate part that presses on the urinary canal, with the prostate capsule around the urinary canal) is completely removed.
If open prostate surgery is performed very well, the entire bleeding adenoma can be removed and there will be no recurrence. If it is not done well, the part may remain and cause problems in the future. Other disadvantages of open surgery are bleeding, prolonged catheterization and prolonged hospitalization.
Another frequently used surgical method in BPH patients is transurethral prostate resection (TUR, TUR-P, closed prostate surgery). In this surgery, prostate adenoma is removed with a closed method by entering through the urinary canal. In patients with very large prostates, it is not possible to remove the entire prostate with the TUR technique.
Especially in TUR operations performed by surgeons who are not very experienced, recurrence is common. Prostatic Hyperplasia complaints begin again in patients who relapse, and some require reoperation.
However, with the HoLEP method, enlarged prostate tissues can be completely removed by separating them from the prostate capsule (the membrane surrounding the prostate). In this way, as a result of the complete removal of the prostate adenoma (enucleation), there is no recurrence or recurrence, or it happens very often. In addition, with the HoLEP method, bleeding is less and the patient is hospitalized less often.
To summarize:
During HoLEP surgery, the prostate adenoma is completely stripped from the prostate capsule, as in open prostate surgery. Therefore, there is no recurrence. In addition, all the removed parts are sent for pathological examination and if there is cancer, it will be revealed.